
Understanding insurance isn’t easy for any of us- not as consumers when we are trying to navigate our own health care and not as providers as we try to figure out how to treat patients within the somewhat arbitrary rules and regulations set by insurance companies.
There are a handful of basic definitions that will help you (and your patients) along the way.
- Deductible: Some insurance policies are subject to a deductible that is determined by the contract with an individual provider. If a patient has a deductible to meet, they are responsible for the “full allowable” until the deductible is met. Once the deductible is met, there may still be a co-insurance (usually a percentage of the daily charges) required but this is typically a much lower cost to the patient. Deductibles and co-insurance amounts may vary slightly based on the number and type of units charged at each visit.
- Co-Insurance: This is a percentage of the billed amount that the patient is responsible for at the time of service. Some policies will require the deductible to be met before the co-insurance goes into effect.
- Co-Payment: This is a flat fee required at the time of service. Co-payment is determined by the insurance provider based on the individual contract. In the case of a co-payment, the patient owes the same amount regardless of the duration of treatment or which codes are billed.
- Full Allowable: This is a predetermined amount based on the contract between the clinic where the patient is treated and the insurance provider. Full allowable is based on the amount the insurance company has agreed to pay for each unit of any given CPT code.
- Out of Pocket Maximum (OOP): This is determined by the individual contract with the insurance provider and is the maximum amount of money a patient will be required to pay (typically in a calendar year). Once the OOP max has been met, services will be covered by the insurance provider at 100%.
- Out of Network (OON): Insurance companies have a network of providers who they contract with. Costs associated with seeing in-network providers are typically lower than seeing OON providers.Some policies may not cover OON providers at all. OON providers generally collect at the time of service and can set their own fee schedules. These providers tend to encourage patients to self-submit invoices to their insurance company for reimbursement of their costs if they have OON benefits available.
Understanding CPT Codes and payment: These are Common Procedural Terminology (CPT) codes that are used among all medical providers that all have a value. For the most up-to-date information on CPT codes you should refer to the American Medical Association’s guide.
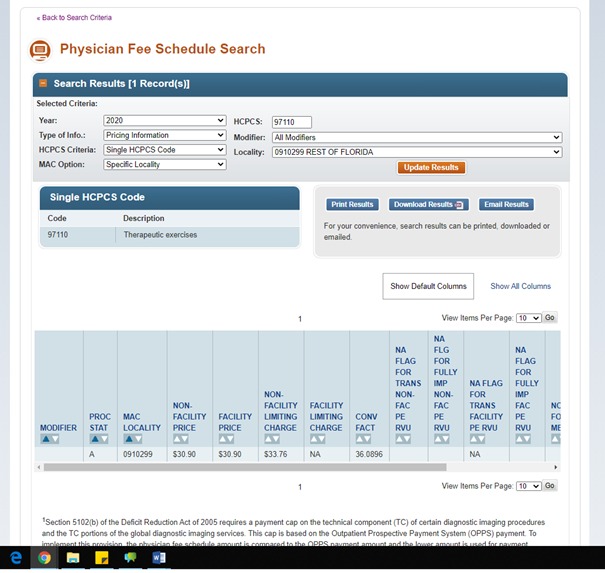
These groups of codes are used to describe tests, surgeries, evaluations, and any other medical procedure performed by a healthcare provider. There are 1000’s of codes but for rehabilitation services, we are mostly concerned with 97000-97999. The value for these codes can be looked up using the CMS Physician Fee Schedule which you can find here: https://www.cms.gov/apps/physician-fee-schedule/search/search-criteria.aspx.
Once you access the tool:
- Enter the CPT code in the box labeled “HCPCS”
- Select “all modifiers” in the box labeled “modifiers”
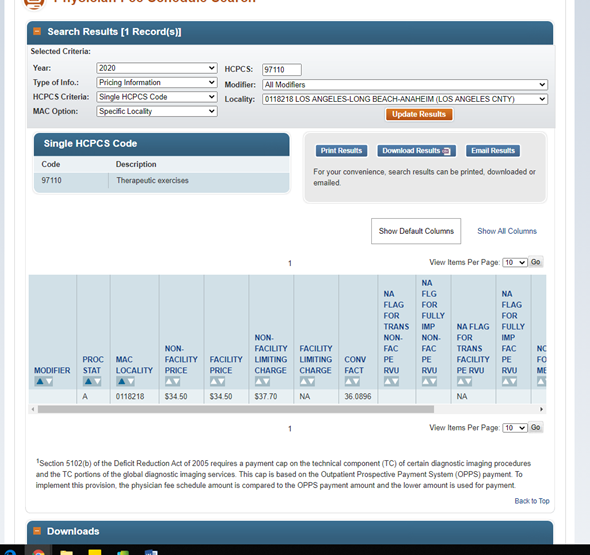
- Select your location (or the closest area to you) in the box labeled “MAC locality”
When you submit this combination of information, you will get a value for the code. For example, in “rest of Florida” which is the closest descriptor for my location in Gainesville, 1 unit of 97110 (therapeutic exercise) is valued at $30.90 while in Los Angeles County, the same code is valued at $34.50.
It is important to note that these are the values assigned by CMS- not individual payers so the actual value in your clinic might be a little different. In reality, we get $32.13 per unit in my clinic from Medicare (in what is really information for another post, we only get $20.72 from most BCBS and an atrocious $8.18 from another BCBS policy) That said, these will give you a good approximate cost.
For now, let’s go back to our original estimate for “rest of Florida” and look at how deductibles, copays and coinsurance change based on this value. If we assume the patient is seen for a full hour and 4 units of 97110 are billed:
- If the patient has a policy that states there is a $1000 deductible and then 20% coinsurance with $1500 OOP max, their cost would be as follows:
- They would pay $123.60 per visit until their deductible is satisfied. After they had paid $1000.00, they would pay $24.72 (20% coinsurance) until their OOP was met. Once they had paid $1500.00, they would be 100% covered by their insurance.
- When they start paying 20%, the insurance company pays the other 80%.
- If the patient has a policy that states they have no deductible and a 20% coinsurance with a $500 OOP max, their cost would be as follows:
- They would pay $24.72 (20%) until they had paid $500 while their insurer pays the other 80%. After $500 the insurer covers 100% of their costs.
- If the patient has a policy that has a $40 copayment, they will owe $40 every visit regardless of what you do (unless your charges are less than $40, in that case they owe the full amount of the charges).
- The insurer would pay whatever is left toward the contracted rate. For example, in my clinic, we had a contracted rate of $69.00 with Avmed so when the charges exceeded $69.00 the patient paid $40.00/visit, Avmed paid $29.00 and the rest was written off by the business.

Remember, all of these conditions are subject to coverage considerations including visit limits, restrictions on number of units per day, which codes can be billed, need for prior authorization, etc.
How are these values set?
Payment for each code is updated annually based on estimates of the costs associated with performing a service. These costs are calculated using collective data from hospital claims and cost reports nationwide. Payments for procedures are adjusted for geographic wage variations using the CMS wage index: 60% of the estimated cost is multiplied by the wage index and added to the remaining 40% of the amount.
Using this information it should be relatively easy to understand why the codes for aquatic therapy and therapeutic activities are reimbursed at a higher rate than therapeutic exercise. In theory, it is more difficult to provide these services so the associated costs are higher and thus reimbursement is too.
This should also make some sense in terms of why reimbursement (and salary) varies based on region- in places where patients make more money, they are charged more for services which translates to higher payments to the clinics and hopefully, higher salaries for therapists.
Why does using different CPT codes matter?
Because most of us are still trying to run a business. Or atleast work for a business that we expect to pay us which means we can’t ignore the profit side of healthcare. Salaries are based on more than what you bill out/collect as an individual therapist- the clinic’s overhead (rent/mortgage, utilities, equipment, legal counsel, non-clinical staff (ie. non-revenue positions), EMR, electronics, etc) has to be factored into the equation too. Simply, if I bill out $100/hr, I can’t also make $100/hr because the rest of the clinic’s bills for that hour need to be paid too.
While it is easier to just bill 4 x 97110, it’s not always in the best interest of the clinic. Several exercises can be classified into more than one code. For example, if you were helping a patient improve their sit to stand transfer, you might use a bridge as:
- therapeutic exercise to improve glute strength to get up and down from a chair (97110)
- neuromuscular re-education to teach the patient what full hip extension feels like so that this skill can be transferred to a sit to stand (97112)
- therapeutic activity to help a patient rise from sitting to standing to get up from a chair/toilet (97530)
All of these are correct uses of the exercise and appropriate billing, however the reimbursement changes based on the intent of the exercise.
97110- $20.72/unit
97112- $21.84/unit
97530- $21.84/unit
If we were working on a hip hinge in the pool for the same reason (to rise from sitting to standing), we would be paid $23.80/unit.
*Remember these rates are unique to our clinic but any clinic will have similar differences in price per unit based on code.
Obnoxious documentation reminder: The caveat to this part of billing is that your documentation must match your billing- and that goes all the way back to your initial evaluation. There should be documentation of decreased glute strength AND difficulty getting up from a chair. The functional activity may have been observed during your session but if it wasn’t, this could still be in your documentation as part of a goal based on a subjective report or an outcome measure.
If your initial evaluation has the necessary information, your notes should be specific about what you’re doing, why you’re doing it and how it helps the patient reach their goals. This does not have to be in every daily note but it does have to be in progress notes at a minimum.
Let’s look at the big picture. If you see 200 patients a month (10/day) and you charge them all 4 x 97110, you will bill out $828.80/day and $16, 576.00/month. If you see the same 10 patients/day and bill out 2 x 97110 and 2 x 97112 you will bill out $850.80/day and $17,016.00/month. While the difference in these values ($1.12/unit) doesn’t seem all that meaningful in a single patient, when you extrapolate out to a day or month you can see how this can make a huge difference ($440/month per therapist or $5,280.00/year per therapist) in the profitability of a business.
